Reading time: 9 minutes | Audience: Support Coordinators, Participants & Families | Updated: April 2026
Occupational therapy and physiotherapy are both allied health disciplines, both funded through Capacity Building — Improved Daily Living in an NDIS plan, and both work with people with disabilities to improve function. So what is the difference — and how do you know which one your participant actually needs?
The confusion is understandable. The two disciplines overlap significantly in some areas, particularly neurological and musculoskeletal conditions, and a participant may genuinely need both. But they have distinct scopes of practice, different core frameworks, and different primary contributions to NDIS outcomes. Getting the distinction right matters because it affects which referrals you make, in what order, and how you use limited IDL budget most effectively.
This guide explains the practical difference between OT and physiotherapy for NDIS support coordinators — when each is indicated, where they overlap, and how to determine which should take the lead for a given participant and situation.
In this article
- The core conceptual difference
- What occupational therapy focuses on
- What physiotherapy focuses on
- OT vs physio — side-by-side comparison
- Where OT and physio overlap — and how to manage it
- When your participant needs OT
- When your participant needs physiotherapy
- When your participant needs both
- NDIS reports — which discipline produces what
- Frequently asked questions
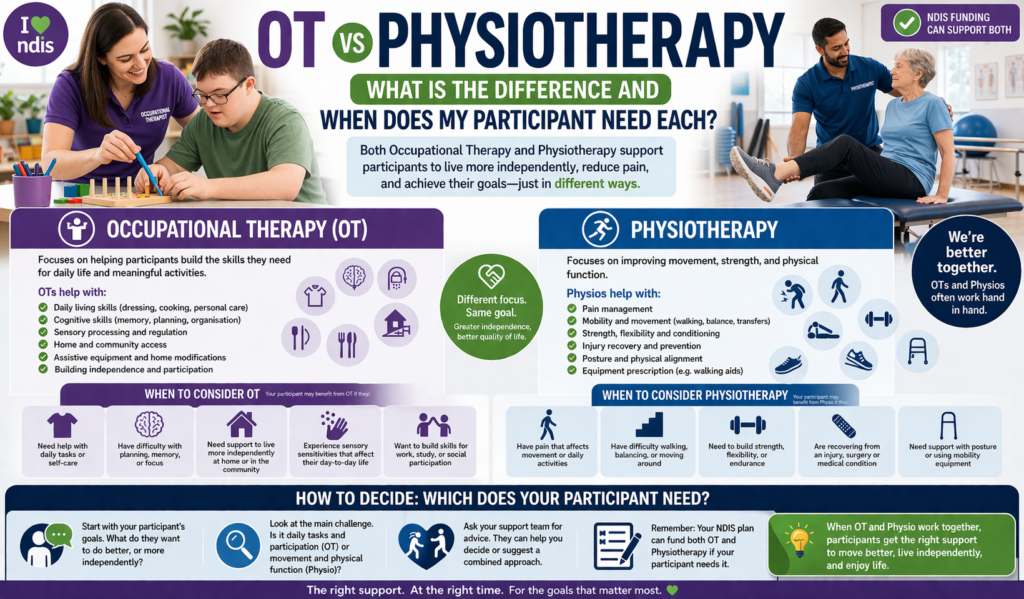
The Core Conceptual Difference
The clearest way to understand the difference between OT and physiotherapy is through their primary questions:
Occupational Therapy asks:
“What can this person do — and what do they want to be able to do?”
OT focuses on participation in the meaningful activities of daily life — the occupations that give life structure and purpose.
Physiotherapy asks:
“How does this person’s body move — and how can we improve that movement?”
Physiotherapy focuses on physical function — movement, strength, mobility, pain, and the integrity of the musculoskeletal and neurological systems.
Put another way: physiotherapy addresses the physical capacity to perform movement. OT addresses the participation in daily activities — using physical capacity, along with cognitive, sensory, and environmental factors, to achieve functional outcomes that matter to the person.
In practice, this means that physiotherapy and OT often address related problems from different angles — and for many participants, the most effective approach involves both disciplines working in coordination.
What Occupational Therapy Focuses On
Occupational therapists address the full spectrum of factors that affect a person’s participation in daily life — physical, cognitive, sensory, emotional, and environmental. OT’s scope includes:
- Daily living skills — showering, dressing, meal preparation, medication management, household tasks, money management
- Cognitive function — memory aids, organisational systems, executive function strategies, safety assessment
- Sensory processing — sensory diets, sensory integration, environmental modification for sensory needs
- Assistive technology — assessment, prescription, and training for wheelchairs, communication devices, daily living aids, environmental control
- Home modification — assessment and clinical justification for accessibility modifications
- School and workplace participation — assessment and strategies for participation in education and employment
- NDIS report writing — Functional Capacity Assessments, SIL assessments, AT prescriptions, home modification reports that underpin NDIS plan funding
- Upper limb rehabilitation — hand therapy, splinting, fine motor retraining after injury or neurological event
- Fatigue management — energy conservation programs and pacing strategies for neurological and chronic conditions
- Social participation and community access — building the skills and environmental supports for meaningful community engagement
What Physiotherapy Focuses On
Physiotherapists address physical function — the body’s capacity to move safely, strongly, and with endurance. Physiotherapy’s scope includes:
- Mobility and gait — walking ability, balance, and safe movement in the community
- Strength and endurance — exercise programs to build the physical capacity for daily activities and community participation
- Pain management — assessment and treatment of pain related to musculoskeletal conditions, neurological conditions, or post-injury
- Neurological rehabilitation — motor retraining after stroke, spinal cord injury, or traumatic brain injury, focusing on movement recovery and compensation
- Respiratory physiotherapy — breathing exercises, airway clearance, and respiratory management for conditions affecting the lungs
- Hydrotherapy — therapeutic exercise in water, particularly for conditions where land-based exercise is limited by pain or weakness
- Post-surgical rehabilitation — recovery programs after orthopaedic surgery, joint replacement, or spinal surgery
- Falls prevention — balance assessment, vestibular rehabilitation, and exercise programs targeting falls risk
- Manual therapy — joint mobilisation, massage, and hands-on techniques for musculoskeletal conditions
- Sports and exercise rehabilitation — conditioning programs for participants with disability who want to maintain physical fitness
OT vs Physio — Side-by-Side Comparison
| Area | Occupational Therapy | Physiotherapy |
|---|---|---|
| Primary focus | Participation in meaningful daily activities | Physical movement, strength, and mobility |
| Core question | What can this person do in their daily life? | How does this person’s body move? |
| Domains addressed | Physical, cognitive, sensory, environmental, social | Physical — musculoskeletal, neurological, cardiorespiratory |
| Assessment environment | Home, school, workplace, community — wherever the activity occurs | Clinic, gym, hydrotherapy pool, home |
| NDIS report types | FCA, AT prescription, home modification, SIL assessment, SDA eligibility | Functional reports (less commonly used for NDIS plan decisions); may contribute to FCA as part of multidisciplinary team |
| AT prescription | Prescribes most categories of AT including wheelchairs, hoists, communication devices, daily living aids | May contribute to mobility aid selection alongside OT; generally does not prescribe complex AT independently |
| Home modification | Assesses and specifies home modifications for NDIS Capital Supports | Does not typically produce home modification reports for NDIS |
| Cognitive and sensory | Core OT scope — memory, executive function, sensory processing, regulation | Not within physiotherapy scope |
| Pain management | Addresses how pain affects participation; fatigue management; adaptive equipment | Direct pain treatment — manual therapy, exercise, electrotherapy |
| Falls prevention | Home hazard assessment, environmental modification, adaptive equipment | Balance training, strength programs, vestibular rehabilitation |
| NDIS funding source | CB — Improved Daily Living | CB — Improved Daily Living |
Where OT and Physio Overlap — and How to Manage It
The areas of genuine overlap between OT and physiotherapy are worth understanding precisely, because overlap creates the risk of duplication — two providers billing from the same IDL budget for work that could be done by one — as well as the risk of gaps, where each discipline assumes the other has addressed something and neither does.
Upper limb function after stroke or neurological injury
This is the most common area of genuine clinical overlap. Both OTs and physiotherapists can deliver upper limb rehabilitation after stroke or brain injury — physiotherapy through motor retraining and strengthening, OT through functional task practice and splinting. In practice, the physiotherapist typically focuses on restoring movement capacity while the OT focuses on using that movement for functional daily tasks. Both contribute; the OT typically takes the lead in translating motor gains into daily activity participation.
Mobility aid prescription
For simple mobility aids (walking frames, crutches, basic manual wheelchairs), physiotherapists frequently assess and prescribe. For complex mobility aids — particularly powered wheelchairs, tilt-in-space systems, and specialised seating — an OT with AT experience typically leads the prescription, with physiotherapy input on positioning and postural needs. For the NDIA’s purposes, complex AT prescriptions for wheelchairs are expected to come from an OT.
Falls prevention
Falls prevention involves both disciplines but from different angles. Physiotherapy addresses the physical determinants of fall risk — balance, strength, vestibular function. OT addresses the environmental and cognitive contributors — home hazards, medication effects on balance, unsafe footwear, cognitive changes affecting judgment. A comprehensive falls prevention program for a high-risk participant should involve both.
Functional capacity in musculoskeletal conditions
For participants whose primary disability is a musculoskeletal condition — significant arthritis, chronic back pain, or post-amputation — both OT and physiotherapy may contribute to an FCA. Physiotherapy assesses physical capacity and pain; OT assesses how that physical capacity translates to (or is limited in) daily activities. The FCA itself is produced by the OT.
Coordinate, don’t duplicate. When a participant has both OT and physiotherapy in their plan, ensure the two providers communicate. A physiotherapist who works on gait training without knowing what the OT is doing around home modification and mobility aids, and an OT who develops a fatigue management program without knowing the physiotherapist’s exercise plan, are each operating at reduced effectiveness. A brief shared care plan or regular communication between providers significantly improves outcomes.
When Your Participant Needs OT
Refer to an OT when the primary concern is:
When Your Participant Needs Physiotherapy
Refer to a physiotherapist when the primary concern is:
When Your Participant Needs Both
Many participants with complex or progressive disabilities genuinely benefit from both OT and physiotherapy — not duplicating each other but working in a complementary, coordinated way. Here are the most common scenarios where both are clearly indicated:
| Participant situation | Physiotherapy contributes | OT contributes |
|---|---|---|
| Stroke rehabilitation | Gait retraining, motor recovery, balance, lower limb function | Upper limb function, ADL retraining, cognitive rehabilitation, home modification, AT, FCA |
| Multiple sclerosis | Strength, endurance, balance, spasticity management, gait | Fatigue management, ADL adaptation, AT, home modification, FCA for plan review |
| Parkinson’s disease | Gait, freezing strategies (physical), balance, LSVT BIG therapy | ADL adaptation, fatigue management, AT (powered mobility, adapted equipment), home modification, FCA |
| Spinal cord injury | Respiratory function, strength, transfer technique, skin integrity, standing program | Upper limb function, AT prescription (complex wheelchair), home modification, daily living skills, FCA, SIL assessment |
| High fall risk — older participant with disability | Balance retraining, strength program, vestibular assessment | Home safety assessment, environmental modification, mobility aid, medication review contribution, cognitive safety |
| Cerebral palsy (adult) | Spasticity management, pain, strength, mobility, hydrotherapy | Daily living skills, AT prescription, home modification, fatigue management, employment support, FCA and SIL if needed |
NDIS Reports — Which Discipline Produces What
One of the most practically important distinctions for support coordinators is understanding which reports and clinical documents each discipline produces — because this directly affects who you need to refer to when specific NDIS funding applications are being prepared.
NDIS report responsibilities by discipline
Produced by OT only:
- Functional Capacity Assessment (FCA)
- Assistive Technology assessment and prescription report
- Home Modification assessment and specifications
- SIL assessment and 28-day roster
- SDA eligibility assessment and report
- Cognitive capacity assessment (often jointly with neuropsychologist)
Produced by physiotherapy:
- Physiotherapy assessment and treatment reports
- Exercise and rehabilitation program summaries
- Falls risk assessment reports
- Hydrotherapy program reports
- Respiratory function reports
May be produced by either or collaboratively:
- Simple mobility aid assessment (walking frames, manual wheelchairs — physio often leads; complex powered mobility — OT leads)
- Functional assessments contributing to a plan review submission (physiotherapy report can supplement but does not replace an OT FCA)
A physiotherapy report does not replace a Functional Capacity Assessment. When a plan review requires clinical evidence of functional impairment across daily living domains, an OT-produced FCA is what the NDIA expects. A physiotherapy report documenting mobility limitations is valuable supporting evidence — but it does not provide the holistic daily living assessment that an FCA delivers. If a plan review is approaching, commission an OT for the FCA even if a physiotherapy report already exists.
NDIS Registered — WA · NT · QLD · VIC
OT referrals for your participants — Darwin, Perth, Brisbane & Victoria
TEAH’s occupational therapists deliver FCA, AT assessment, home modification, SIL assessment, and individual OT therapy across all locations — with low wait times and NDIA-quality reports.
Frequently Asked Questions
Can OT and physiotherapy be funded at the same time from the same NDIS budget?
Yes. Both OT and physiotherapy are funded from Capacity Building — Improved Daily Living, and a participant can access both simultaneously, as long as the total IDL budget is sufficient to cover both providers’ claims. Ensure the plan includes enough IDL for the combined therapy load before committing both providers.
Can a physiotherapist write an FCA for NDIS plan review?
No. The NDIA expects Functional Capacity Assessments to be produced by occupational therapists. While physiotherapists can produce valuable functional reports documenting physical capacity and mobility, these do not substitute for an OT FCA for plan review purposes. If a plan review is approaching, an OT-produced FCA is required.
My participant has both OT and physio in their plan but I’m not sure who does what. How do I sort this out?
Convene a brief case conference — even a 15-minute call — between the OT and physiotherapist. Ask both to share their current goals for the participant and identify any overlap or gap. Where both are working on related areas (upper limb function after stroke is a classic example), agree on who leads each component and how they will communicate progress. A brief shared care plan prevents duplication and ensures both providers are working toward complementary rather than conflicting goals.
My participant’s GP has referred them to a physiotherapist, but I think they need an OT. Can I still refer to an OT independently?
Yes. GP referrals are not required for NDIS-funded OT, and a GP’s recommendation of one discipline does not preclude referral to another. If the participant’s NDIS goals and functional needs indicate OT, refer directly. You may wish to share the OT’s assessment findings with the GP once available, particularly if the findings have implications for the participant’s medical care.
A participant with MS already sees a physiotherapist — do they also need an OT?
Almost certainly yes, if they do not have a current FCA. For MS participants, physiotherapy addresses physical function — strength, balance, gait, and spasticity. OT addresses fatigue management, daily living adaptations, cognitive changes, home modification, AT prescription, and NDIS plan review documentation. These are distinct contributions that a physiotherapist cannot substitute. The FCA alone is sufficient justification for an OT referral alongside existing physiotherapy.
Does TEAH provide physiotherapy as well as OT?
Yes — TEAH provides occupational therapy, speech pathology, and physiotherapy across Darwin (NT), Perth (WA), Brisbane (QLD), and Victoria. If your participant needs both OT and physiotherapy, referring to TEAH for both allows the two disciplines to coordinate within the same organisation — reducing communication overhead and improving continuity of care. Contact our intake team on 1300 203 059 to discuss multi-discipline referrals.
Summary
OT and physiotherapy are complementary disciplines that address different — though related — aspects of disability and daily function. Physiotherapy focuses on the body’s physical capacity to move. OT focuses on how that capacity (combined with cognitive, sensory, and environmental factors) translates into participation in the activities of daily life.
For NDIS purposes, the distinction matters practically: OT produces the FCA, AT prescription, home modification, and SIL reports that drive plan funding decisions. Physiotherapy contributes valuable functional information but does not produce these documents. When both are needed, coordinate them — a physiotherapist and OT working in parallel without communication is less effective than the same pair working from a shared understanding of the participant’s goals.
TEAH provides both OT and physiotherapy across Darwin, Perth, Brisbane, and Victoria — making coordinated multidisciplinary referrals straightforward.
Refer for OT or physiotherapy with TEAH
Darwin (NT) · Perth (WA) · Brisbane (QLD) · Victoria
Related articles
- How to refer a participant for an OT assessment — a support coordinator’s guide
- When should I refer my NDIS participant to an occupational therapist?
- OT for neurological conditions — MS, Parkinson’s, and stroke
- OT for acquired brain injury — what NDIS participants need to know
- Our Occupational Therapy Services — Darwin, Perth, Brisbane & Victoria
TEAH Allied Health Team
Top End Allied Health (TEAH) is an NDIS-registered allied health provider delivering occupational therapy, speech pathology, physiotherapy, and supported accommodation across WA, NT, QLD, and Victoria. Referrals: referrals@topendalliedhealth.com.au | 1300 203 059